In Uganda, while complementary feeding is culturally accepted, there is limited published information on specific cultural practices and their influence on feeding behaviors among children. This study assessed feeding practices, maize purchasing patterns, and reported weights and heights among children aged six to 24 months in Kassanda-road and Myanzi villages, Kassanda District, Central Uganda. A cross-sectional survey was administered to mothers (N=119) in the two villages. All mothers completed the survey with 56.3% and 43.7% from Kassanda-road and 43.7% Myanzi villages, respectively. More than half of the mothers (58.8%) were between 18 to 25 years of age. Of the mothers, 33.6% reported having high school education, while at least one in three mothers reported having primary level or no formal schooling. Roughly 59.7% of the mothers reported monthly earnings of less than US$55 (200,000 Ugandan shillings). During breastfeeding, 77.3% of mothers reported consuming predominantly cereals as 'special' foods. Although 70.6% of mothers reported exclusive breastfeeding for six months, 53.4% introduced water before six months. The majority (82.9%) of mothers reported giving water to their children to prevent constipation. The mothers reported that they breastfed because of its nutritional value (38.6%) and cost-effectiveness (23.0%). Common complementary foods included mashed potatoes and cereal porridge, with maize-millet blend porridge being the most frequently consumed (39.5%). Maize was predominantly sourced from local retail shops (43.7%) and household gardens (31.9%). Mothers reported feeding maize porridge and maize-blend porridge twice daily (42.0% and 33.6% respectively), with daily consumption of one (43.0%) to two cups (31.6%) of maize porridge. Most (85%) children had normal BMI, with 3% and 13% underweight and overweight/obesity, respectively. Overweight was higher in the girls (16%) than the boys (10%). Overweight/obesity rates were higher in Myanzi village (15%) compared to Kassanda-road village (10%).
*Corresponding Author:
Adelia C. Bovell-Benjamin
Department of Food and Nutritional Sciences, Tuskegee University Tuskegee, Alabama, 36088, USA; Tel: +1-(334) 727-8717; Email: abovellbenjamin@tuskegee.edu
ABSTRACT
In Uganda, while complementary feeding is culturally accepted, there is limited published information on specific cultural practices and their influence on feeding behaviors among children. This study assessed feeding practices, maize purchasing patterns, and reported weights and heights among children aged six to 24 months in Kassanda-road and Myanzi villages, Kassanda District, Central Uganda. A cross-sectional survey was administered to mothers (N=119) in the two villages. All mothers completed the survey with 56.3% and 43.7% from Kassanda-road and 43.7% Myanzi villages, respectively. More than half of the mothers (58.8%) were between 18 to 25 years of age. Of the mothers, 33.6% reported having high school education, while at least one in three mothers reported having primary level or no formal schooling. Roughly 59.7% of the mothers reported monthly earnings of less than US$55 (200,000 Ugandan shillings). During breastfeeding, 77.3% of mothers reported consuming predominantly cereals as 'special' foods. Although 70.6% of mothers reported exclusive breastfeeding for six months, 53.4% introduced water before six months. The majority (82.9%) of mothers reported giving water to their children to prevent constipation. The mothers reported that they breastfed because of its nutritional value (38.6%) and cost-effectiveness (23.0%). Common complementary foods included mashed potatoes and cereal porridge, with maize-millet blend porridge being the most frequently consumed (39.5%). Maize was predominantly sourced from local retail shops (43.7%) and household gardens (31.9%). Mothers reported feeding maize porridge and maize-blend porridge twice daily (42.0% and 33.6% respectively), with daily consumption of one (43.0%) to two cups (31.6%) of maize porridge. Most (85%) children had normal BMI, with 3% and 13% underweight and overweight/obesity, respectively. Overweight was higher in the girls (16%) than the boys (10%). Overweight/obesity rates were higher in Myanzi village (15%) compared to Kassanda-road village (10%).
Keywords: Maize purchasing practices; feeding practices; complementary feeding; maize consumption; body mass index.
ABBREVIATIONS
IYCF Infant and young child feeding
CF Complementary Feeding
EBF Exclusive Breastfeeding
CDC Centers for Disease Control and Prevention
BMI Body Mass Index
WHO World Health Organization
INTRODUCTION
The first two years of a child's life are important for establishing lifelong health and optimizing growth through nutrition [1-2]. Infant and young child feeding (IYCF) practices include breastfeeding, complementary feeding (CF), and other practices that ensure children get adequate nutrition [1-2]. The recommended IYCF practices include breastfeeding, CF, diet diversity and meal frequency [1-2]. Briefly, IYCF indicators for breastfeeding include ever breastfed, early breastfeeding initiation, exclusive breastfeeding (EBF) for first two days after birth and under six months, respectively, mixed milk feeding less than six months and continued breastfeeding for 12 to 23 months [1]. The CF indicators include the introduction of solid, semi solid or soft foods at six to eight months. For children six to 23 months, recommendations are a minimum diversity diet, minimum meal frequency, milk feeding frequency for non-breastfed children, and egg and/or flesh food consumption [1]. Bottle feeding is another IYCF indicator [1].
The World Health Organization (WHO) recommends EBF for the first six months of life for healthy infant growth [1]. However, as the child’s nutritional demands increase after this period, breast milk alone becomes insufficient, necessitating the introduction of CF to support growth and development [3]. CF, which is the introduction of foods and liquids other than breast milk, plays a crucial role in IYCF, and significantly influences children's nutritional status [4]. It has been estimated that in Uganda, malnutrition contributes up to 60% of child mortality [5]. Although breastfeeding is widely accepted in Uganda, the rate of EBF remains low [6]. National data indicate that approximately 10% of infants under six months are EBF, with variations observed across different regions [7,8]. Moreover, a high proportion of mothers in Uganda do not adhere to recommended IYCF practices, highlighting notable gaps in the timely introduction and adequacy of CF [9]. Persistent concerns include inadequate meal frequency and limited dietary diversity [10-11].
In Uganda, many factors contribute to non-compliance with international IYCF guidelines, such as limited support for women in healthcare settings and communities, cultural beliefs favoring mixed feeding, and misconceptions about breastfeeding [12-16]. Issues such as inappropriate timing and irregular frequency of complementary feeding, along with deficiencies in the nutritional quality of traditional complementary foods, further compound these challenges [17-18]. Despite the documented benefits of effective complementary feeding in reducing childhood mortality, suboptimal feeding practices persist in Uganda [19-21].
Appropriate complementary feeding has been shown to reduce stunting, overweight, micronutrient deficiencies and childhood mortality [19-21]. In Uganda, the most commonly used complementary foods include semi-solid preparations made from maize, cassava, sweet potatoes, and yams [22-23]. The increasing availability of processed baby foods and greater female workforce participation negatively impact on breastfeeding and CF practices in Uganda [24-25]. There is limited published literature regarding the cultural beliefs and practices associated with CF among children aged six to 24 months in Uganda [17-18, 26]. The current study is part of a larger study, which investigates mycotoxin exposure in maize-based complementary foods in Tanzania. Overall, adequate CF in Uganda faces multiple barriers, including cultural and traditional beliefs, economic barriers, lack of knowledge and awareness, and limited access to health services. Addressing these challenges requires research to determine the appropriate interventions. It is against this backdrop that the study objective was designed to assess feeding practices, maize purchasing patterns, and reported weights and heights among children aged six to 24 months in Kassanda-road and Myan-zi villages, Kassanda District, Central Uganda.
MATERIAL AND METHODS
The Ethical Consent
Ethical approval for the study was obtained from the Human Participant Review Committee at Tuskegee University and the District Health Office of Kassanda District, Uganda.
Research Setting
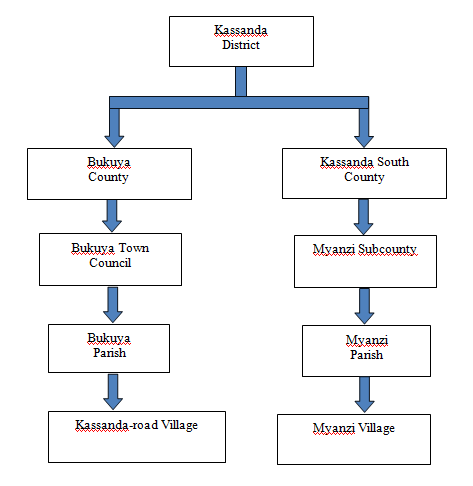
The study was conducted in Kassanda-road and Myanzi villages in the Kassanda District, Uganda (Figures 1-2). Kassanda-road is a peri-urban village, situated in Bukuya county, lies at a latitude of 0°40'28.0"N and a longitude of 31°50'05.0"E (Latitude: 0.674454; Longitude: 31.834716). Myanzi is a rural village located in Kassanda-South county and is positioned at coordinates 0°26'15.0"N, 31°54'38.0"E (Latitude: 0.437501; Longitude: 31.910547).
Research Design
The study was cross sectional.
Questionnaire Development
The survey questions were reviewed by nutrition, dietetics and sociology professionals to ensure that they were ordered, logical, clear, grammatically correct, well formulated, comprehensible and culturally sensitive. The survey was administered by trained interviewers and was completed in 30 minutes.
Survey Instrument
The final survey instrument consisted of 32 items with four sections, namely: demographics, cultural and feeding practices of children, and maize-purchasing practices of the mothers. Mothers provided responses for the children.
Demographics
The demographics section elicited information about the child’s age, gender, and anthropometrics (self-reported heights and weights). Additionally, information regarding the mothers’ age, marital status, education level and income was collected.
Cultural Beliefs
The cultural beliefs section comprised of 10 closed- and one open-ended question(s), which assessed beliefs regarding breastfeeding, as well as complementary feeding. Responses to these questions were recorded as multiple-choice options, as well as a modified 3-point Likert-type scale adapted from Klymchuk and colleagues [27]. Participants indicated their agreement level with statements as '1=Agree,' '2=Disagree,' or '3=Do not know.’
Feeding practices
This section consisted of eleven closed-ended questions, which evaluated feeding practices regarding complementary feeding (type, quantity, and frequency of complementary foods consumed). The questions were recorded using multiple-choice responses.
Maize Purchasing Practice
This section consisted of a single close-ended question which elicited information on points of purchase of maize.
Participant Recruitment
Mothers were recruited on vaccination days at Kassanda-road and Myanzi Health Centers, with the support of nursing staff. The study was explained to the mothers and those who agreed to participate gave their oral consent. The selection criteria were limited to: i) mothers aged 18 to 50 years, and ii) mothers with children aged six to 24 months.
Data analysis
Data were analyzed using Statistical Package for Social Sciences software (SPSS version 21 for Windows, IBM, New York, US). Descriptive statistics including means, frequencies, and percentages, were determined for various participant responses. The anthropometric data were analyzed using the Centers for Disease Control and Prevention (CDC) Children and Teen BMI Calculator [28].
RESULTS
Demographics
The demographic characteristics of the participants are presented in Table 1. In total, 119 mothers participated, with 56.3 and 43.7% from Kassanda-road and Myanzi villages, respectively. More than half (58.8%) of the mothers were between 18 to 25 years old. Table 1 also provides information on the ages, number, and percentage of children included in the survey. Of the mothers, 33.6% reported having high school education, while at least one in three mothers reported having only a primary level or no formal schooling. The reported family incomes were low, with over half (59.7%) earning less than US$55 or 200,000 Ugandan shillings (Ugshs) per month.
Cultural Beliefs
The majority (89.9%) of mothers agreed that breastmilk was more nutritious than other foods including baby formula (Table 2). A high percentage (77.3%) of the mothers reported eating ‘special foods’ during breastfeeding (Table 2). These foods included cereals, root porridges, beans, and garden eggs, known scientifically as Solanum aethiopicum and locally referred to as ‘Entula’. While 86.5% of the mothers reported exclusively breastfeeding, over half (53.4%) admitted to introducing water before six months of age.
Table 3 shows the reported reasons why mothers breastfed their toddlers in the two villages. Less than half of the mothers reported that they breastfed because breast milk was nutritious (38.6%) and cheap (23.0%). Additionally, a high percentage (67%) of the mothers reported that weaning foods improved children’s growth and wellbeing (Table 4). Furthermore, the majority (82.9%) of mothers reported that they fed their children water to prevent constipation (Table 4).
Feeding Practices
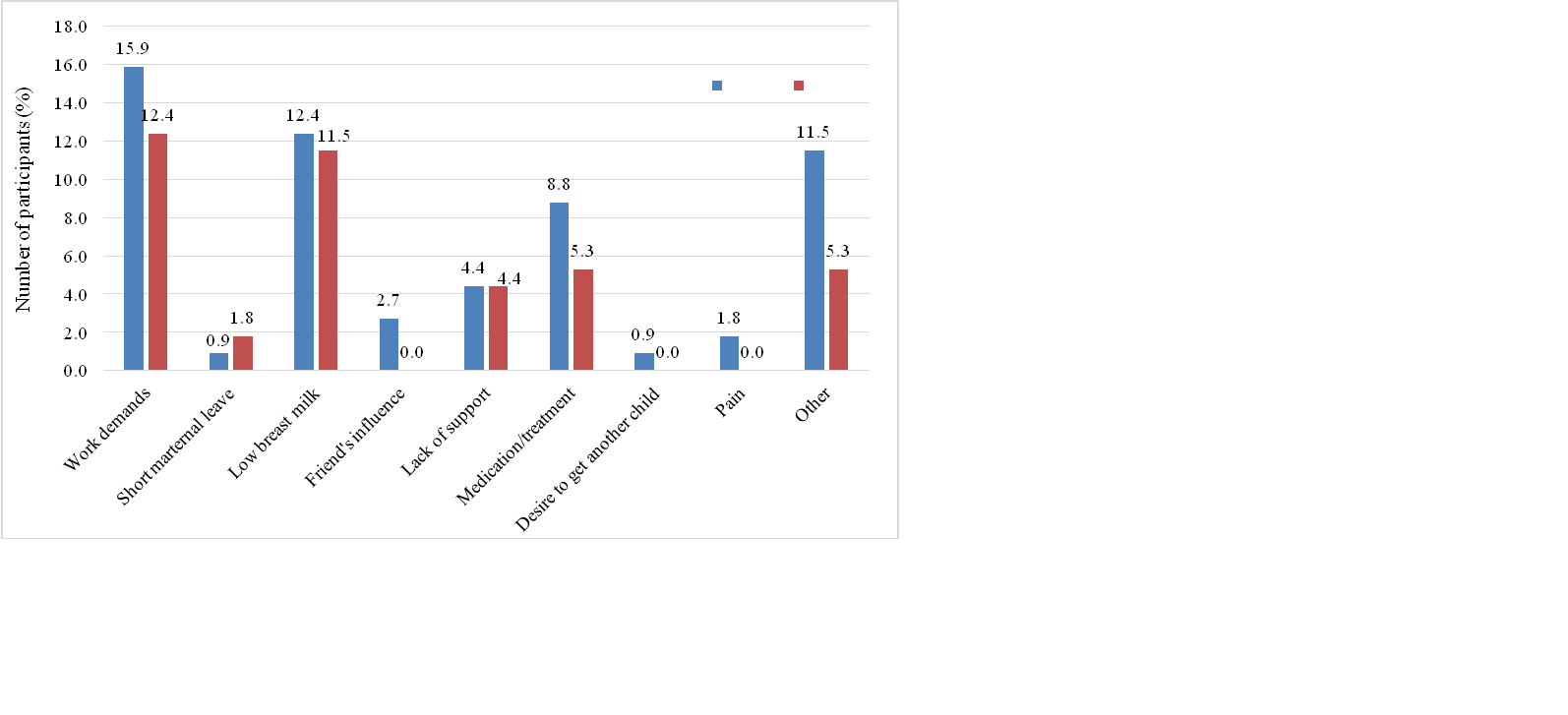
Table 5 illustrates the feeding practices reported for the two villages. The mothers reported breastfeeding for 12 (37.0%) and 24 (36.0%) months. Additionally, the majority (70.6%) of mothers reported initiating CF at six months of age. The commonly reported complementary foods included mashed potato, cereal porridge, and Enkejje soup, often mixed with mashed food. Furthermore, maize-millet blend porridge was the most prevalent (39.5%) cereal porridge blend offered to children, followed by maize-enkejje blend (26.3%). Mothers reported work demands (28.3%) and insufficient breast milk (23.9%) as the primary reasons for starting CF before the age of six months (Figure 3).
The consumption frequency of maize porridge per day was notably high, with 42.0% of the mothers stating that their children consumed maize porridge at least twice daily. Similarly, the consumption frequency of blended porridge per day was also high, with 33.6% of the mothers reporting that their children consumed maize-blended porridge at least twice daily. The highest reported quantity of maize porridge consumed per day was 250 mL or one cup, followed by 500 mL or two cups (Table 6). Moreover, mothers reported a high frequency of water consumption per day for the children (Table 6).
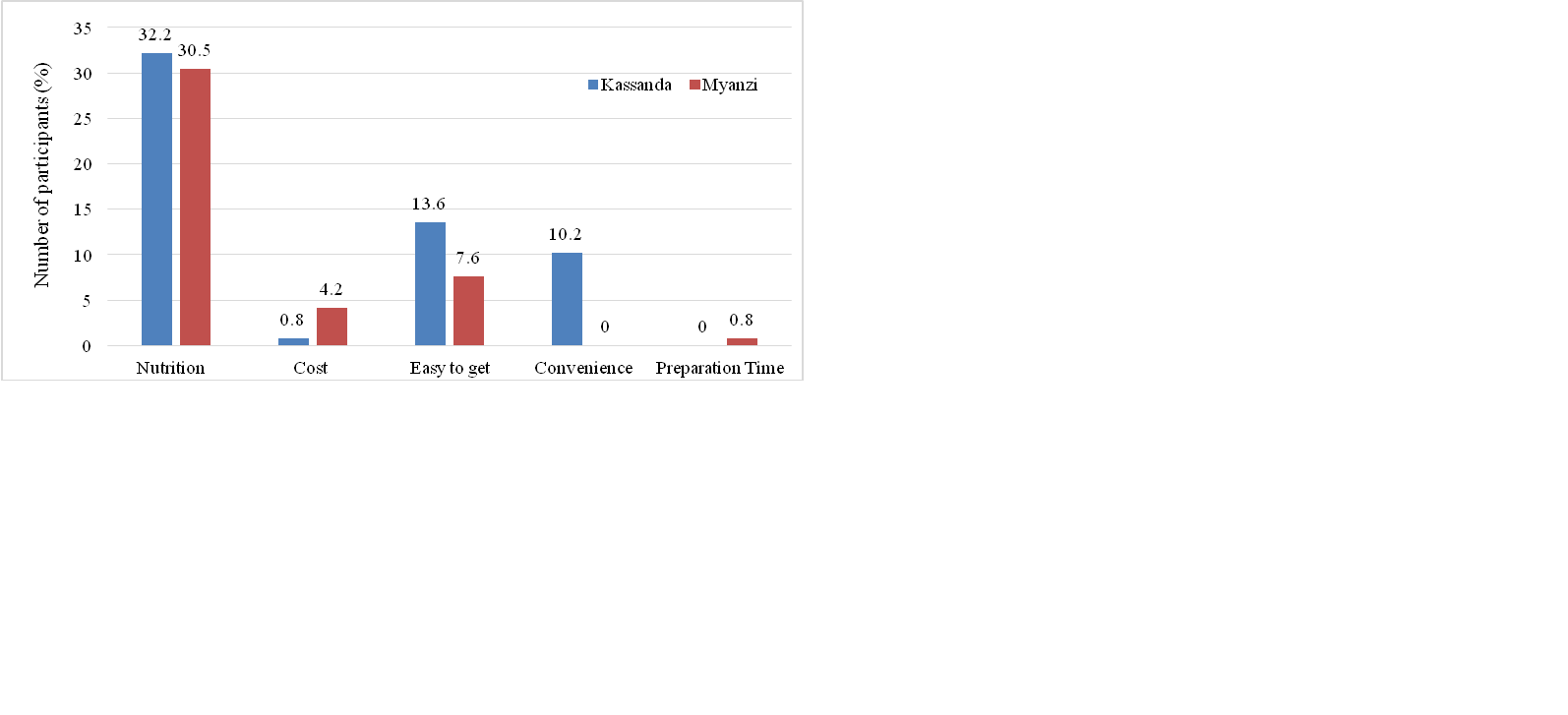
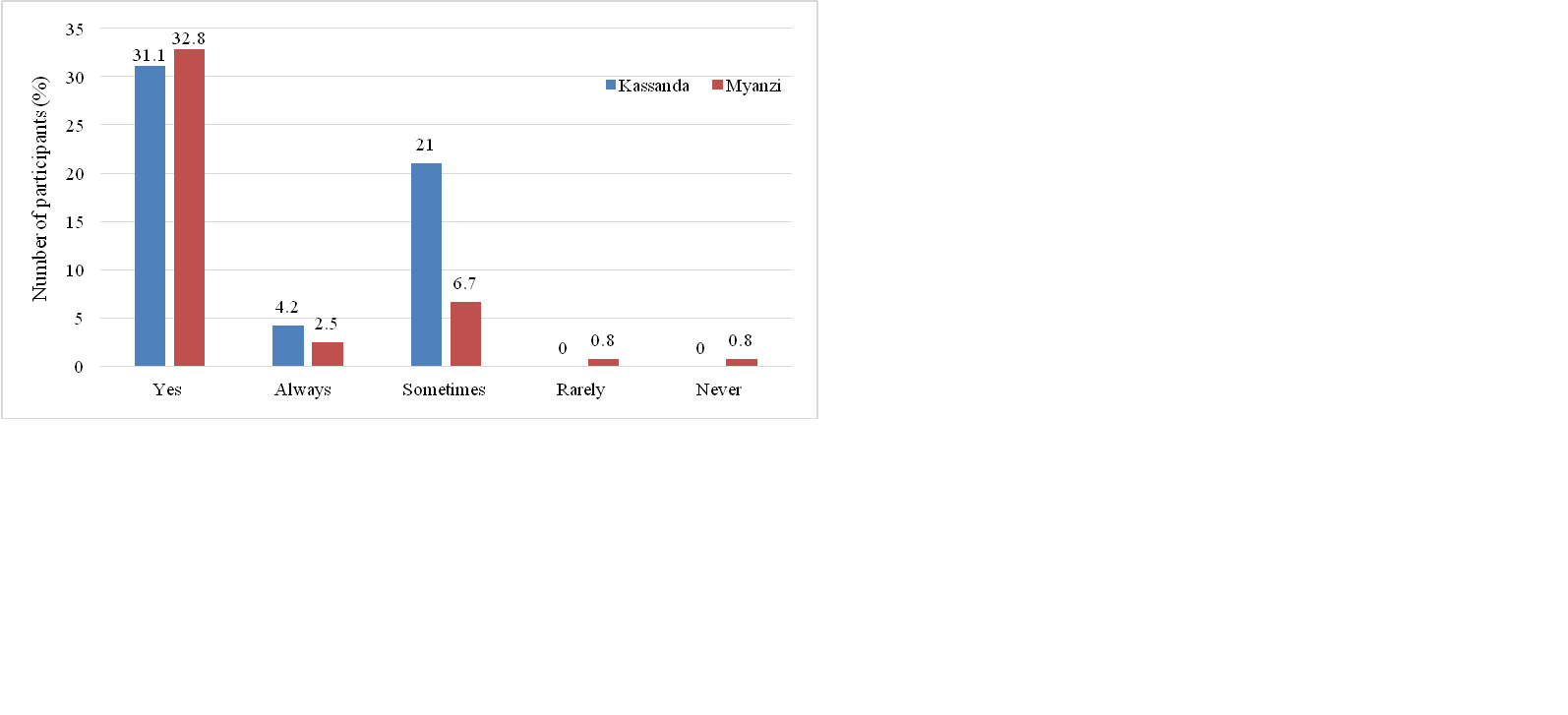
The majority of mothers reported that nutritional value (62.7%) and accessibility (21.2%) were the primary factors influencing their choice of complementary foods for their children (Figure 4). Furthermore, a large percentage of the mothers agreed that nutrition was important (63.9%) or sometimes important (27.7%) (Figure 5).
Reported Weights and Heights
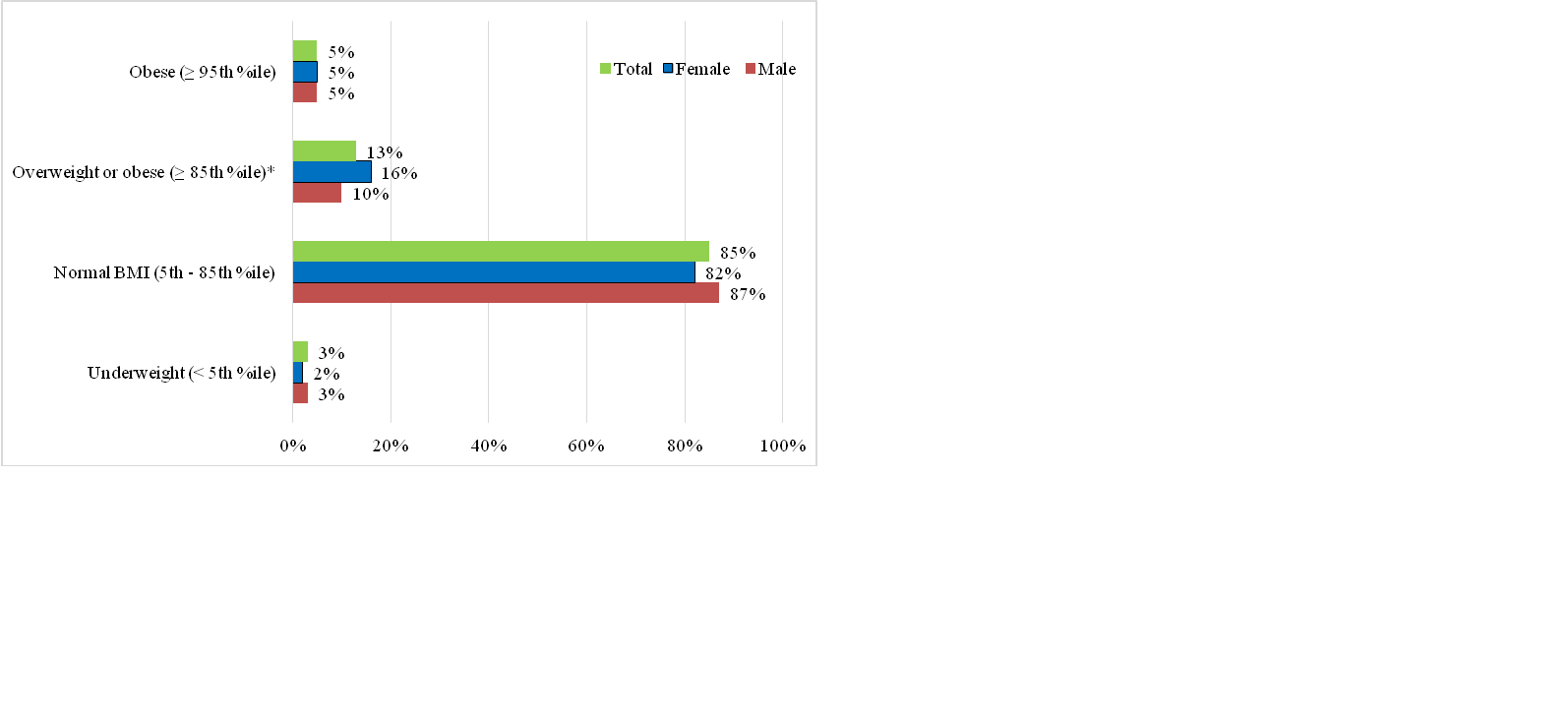
The calculated BMI showed that the majority (85%) of the children had a normal BMI (5-85th percentile) with girls being slightly (16%) more overweight (≥ 85th percentile) than to boys (10%) (Figure 6).
DISCUSSION
Cultural Beliefs
‘Special’ foods
The study revealed that most mothers consumed 'special' foods, predominantly cereals during breastfeeding. While the precise reasons for this practice were not clearly understood, mothers indicated that they believed these foods helped increase breast milk volume. Cultural beliefs and local knowledge are known to influence dietary choices during breastfeeding and CF [14, 29-31]. For example, among the Batwa and Bakiga communities in western Uganda, traditional birth attendants are trusted sources of advice on breastfeeding and CF [3]. Usually, mothers are provided with herbs believed to enhance milk production, and are advised to chew foods to soften it, before feeding it to the children for the initial solid meals [3, 25, 32-33]. In southern Uganda, mothers feed their children Ekyogero (herb) within the first two weeks of life, believing that it made their babies strong, ward off illnesses, and keep them healthy [27]. In Ghana, eggs were avoided during pregnancy due to the belief that they caused overweight in the fetus, leading to complications during childbirth [34]. Culturally, the preference for cereals in the present study aligns with specific beliefs and practices observed in many cultures [35]. The accessibility and affordability of cereals in central Uganda may further explain their preference as a ‘special’ food. In many African cultures, including Uganda, grandmothers play a crucial role in guiding feeding practices, thereby impacting nutrition outcomes and child health [36]. The prevalence of cultural beliefs and food taboos surrounding "special" foods may sometimes hinder the intake of essential nutrients critical during the CF period [37].
Exclusive Breastfeeding
Exclusive breastfeeding (EBF) for the initial 6 months of life, as advised by the World Health Organization (WHO), is widely recognized as a highly effective method to promote children’s optimal growth and development [38]. Children who are exclusively breastfed for this duration demonstrate improved nutritional status, lower incidence of illness, and enhanced early childhood development [39, 40]. The current study revealed discrepancies between the reported high rate of EBF and the practices described by the mothers. For example, although 86.5% of the mothers reported EBF, 52.5% of them gave water to their children before the recommended age of six months. Mothers in this study reported EBF ranging from two (1.8%) to six (53.8%) months. Our findings are in contrast with another study in western Uganda that reported a median duration of EBF of 3.5 months [41]. Similar studies in different regions of Uganda reported varying rates of EBF ranging from as low as 6% in central Uganda to 57% in western Uganda [27]. In Nigeria, Aliyu and others [42] reported that only 40% of mothers practiced EBF in the first six months.
Early introduction of water was reported to prevent constipation and reduce thirst among children, which possibly indicates limited knowledge regarding EBF and its benefits among mothers. Wamani and others [41] reported that 43% of mothers in western Uganda used plain water, glucose water, and sugar water (most common) in the first three days after delivery. Likewise, Engebretsen and colleagues [43] found that 43.5 and 36.4% of mothers in Uganda and Burkina Faso, respectively, introduced liquids such as water and sugar water in the first three days of their children’s birth. Early introduction of water may lead to decreased breast milk consumption, which might possibly expose them to malnutrition and micronutrient deficiencies [44, 45]. Furthermore, water in rural Uganda is prone to contamination, heightening the risk of diarrhea and waterborne diseases [46]. Breast milk comprises over 80% water, and thus adequately meets infants’ hydration needs, even in hot climates [47]. Understanding as well as adherence to recommendations of breastfeeding remain minimal among Ugandan rural mothers [6, 41]. Additionally, the lack of accurate breastfeeding information among healthcare workers in developing countries like Uganda may further impact the breastfeeding messages conveyed to mothers [48]. Therefore, there is a pressing need to enhance breastfeeding and infant feeding education to ensure better understanding and adherence to EBF practices among mothers to optimize child health.
Feeding practices
Breastfeeding practices
Breast milk is widely acknowledged as the optimal source of nutrition for infants, supplying vital nutrients crucial for their healthy growth and development [49]. Additionally, breast milk contains antibodies, which offer immediate protection against various diseases [39]. Also, breastfeeding benefits the mother by serving as a family planning mechanism and reducing the risk of non-communicable diseases such as breast and ovarian cancers [50]. Most mothers in the study reported that they breastfed for a minimum of 12 months. This finding is in agreement with previous research by Bbaale [51], who reported mean breastfeeding duration of 14.1 months in Uganda, with 75% of children breastfed for at least 18 months. In southwest Uganda, 80.8% of mothers continued breastfeeding for more than 12 months [52]. Similarly, Wamani [41] reported a median duration for breastfeeding of 21.3 months in western Uganda. However, the practice of breastfeeding in Uganda falls short of the 87.5% (>12 months) reported among breastfeeding women in Nigeria [42].
Complementary feeding
At six months, breast milk alone is not sufficient to meet children’s energy and nutritional needs, necessitating complementary foods [53]. The mothers in the current study reported that the most common CF was starchy vegetables and maize and grains. This finding is consistent with other research reporting cereal-based gruels as common CF with limited intake of fruits, vegetables, and animal protein [54, 55]. Some mothers in the study reported feeding family meals without specialized CF. This practice could potentially limit nutrient absorption [40]. Maize/maize-blend porridge was the most common CF in Kassanda-road and Myanzi villages, with most mothers feeding their children at least twice a day. This is in line with optimal feeding frequencies as reported by Engebretsen and colleagues [18]. However, dependency on CF mainly from starchy vegetables and grains may contribute to micronutrient deficiencies prevalent among under-fives in Uganda [23]. While fortified CF are recommended, their affordability remains a challenge for rural mothers with low incomes, necessitating the development of sustainable, locally available CF blends [56].
In this study, more mothers reported introducing CF at six months than those in Nigeria and Central Uganda [42, 54]. Similarly, in western Kenya, Mbagaya [57] reported that by age four months, 34.5% of children were receiving CF such as maize/millet porridges. Conversely, findings from eastern Kenya indicated that by age three months, 90% of children were already receiving maize or millet gruels [58]. In the current study, younger mothers reported weaning their children earlier than older mothers. Similar findings were reported in the literature [34]. Ssemukasa [34] speculated that this tendency is possibly due to barriers such as lack of preparedness, experience, and financial dependency on guardians [34]. The early introduction of CF may result from insufficient education on breastfeeding and CF, as observed among Batwa and Bakiga communities in south-western Uganda [3]. Additionally, the need to return to work was cited as another contributory factor to early CF. For instance, in Luweero District, heavy agricultural demands during planting and harvesting seasons, inadequate spousal support and household responsibilities, were reported to impact negatively on mothers’ ability to provide optimal breastfeeding and CF [17].
Anthropometrics
The majority (85%) of children in the current study had BMI within the normal range, with low occurrences of overweight/obesity and underweight. These results are consistent with a similar study, which reported comparable levels of overweight (3.9%) and obesity (1.1%) among children under five years in Uganda [41]. In contrast to the present study, the Uganda Demographic and Health Survey (UDHS) reported a higher national prevalence of overweight and obesity at 11% [59]. Interestingly, the current study revealed more overweight among girls compared to boys, aligning with findings from Kampala where girls had higher rates of overweight (64.4%) compared to boys (35.6%) [60]. In contrast to the present study, research in Eastern Africa indicated that male children under-five were 16% more likely to be overweight than their female counterparts [61]. A higher prevalence of overweight/obesity was observed in Myanzi compared to Kassanda-road village. It can be speculated that this is the outcome of the differing socio-environmental contexts of these villages. Myanzi is a rural village while Kassanda-road is peri-urban. Obesity is substantially more prevalent among rural populations than urban ones. Rural residents tend to more calorie-dense foods as indicated in CF practices in this study and others [62].
STUDY STRENGTHS AND LIMITATIONS
The study's cross-sectional nature provided a snapshot, which captured current behaviors and trends within the two villages in the Kassanda district. This study builds on the knowledge database regarding two villages, which are underrepresented in the existing literature. The current study offers localized data that can inform targeted interventions and policies aimed at enhancing feeding practices and ultimately improving child health outcomes in the Kassanda district in general, and the two villages in particular.
The study collected data at a single point in time, therefore it is difficult to establish causality. Additionally, the study findings were limited to a specific geographical area, therefore the findings cannot be generalized. The sample size was small and not representative of the villages. The feeding practices data collected were based on recall, which could result in over- or under-estimation of actual feeding practices. The strengths of the current study outweigh the limitations. Despite the limitations of the cross-sectional design, the study provided valuable insights and a real-time overview of the CF practices within the two villages in the Kassanda district. The information gathered could be useful in assisting policymakers to identify ‘at-risk’ groups and it also provided information for targeted intervention. To strengthen future research, the study could incorporate longitudinal data collection, a larger and more diverse sample, and direct observation of feeding practices to improve accuracy. Future studies can increase reliability, generalizability, and policy impact, ultimately leading to better-informed interventions to improve infant feeding practices in Uganda and elsewhere.
CONCLUSION AND RECOMMENDATIONS
This study provided valuable insights into feeding practices among children in Kassanda. Mothers reported a high consumption of special foods, particularly cereals, during breastfeeding, and a variety of starchy complementary foods, such as maize-based porridges and mashed vegetables like potatoes. The majority of children had a normal BMI, which suggests that despite economic challenges, many children are maintaining an adequate weight-for-height. Cultural acceptance of CF indicates that existing local feeding practices could be leveraged for nutrition interventions. The early introduction of water contradicts WHO’s recommendations and may increase infection risks due to unsafe water sources. The widespread practice of giving water before six months aligns with cultural norms seen in other African countries but is known to displace breastmilk intake and expose infants to infections. The high reliance on maize-based porridge may increase the risk for micronutrient deficiencies, such as vitamin A, iron and zinc. The higher prevalence of overweight/obesity in Myanzi village versus. Kassanda-road village suggests possible differences in food availability, feeding frequency, or physical activity that require further exploration.
The low-income levels reported in the study might limit access to diverse food options, leading to reliance on maize-based diets. This is consistent with previous studies in Uganda showing that economic constraints influence food choices among rural households. The current study suggests that CF practices may influence BMI, but other factors like physical activity, genetic predisposition, and feeding frequency should be considered. Given that girls had a higher overweight rate than boys, an explanation could be differences in metabolic rates or feeding behaviors.
To advance the discipline and improve IYCF practices, the following recommendations are suggested: i) conduct longitudinal studies to assess the long-term impact of CF on child growth and development and to establish causal relationships between feeding patterns and nutritional outcomes; ii) future studies should analyze micronutrient intake alongside feeding practices and consider evaluating household food security and affordability of alternative nutrient-dense foods; iii) more in-depth investigations into cultural beliefs, such as the reasons behind early water introduction and cereal consumption. Engage with local elders, health workers, and mothers to develop culturally acceptable nutrition interventions; iv) strengthen nutrition education programs on optimal feeding practices, targeting young mothers (18-25 years) and promote affordable, locally available, nutrient-rich CF. Overall, future research should expand geographic coverage, track long-term trends, and incorporate qualitative insights to improve IYCF strategies in Uganda and elsewhere.
ACKNOWLEDGEMENTS
The authors acknowledge the nurses who assisted with the recruitment and interviews, mothers and their children for participating.
REFERENCES
TABLES
Table 1. Socio-demographic Characteristics of the Participants (N=119).
|
Characteristic |
Description |
Village |
Total |
|
|
Kassanda-road |
Myanzi |
|||
|
Mothers’ Age (years) |
18 – 25 |
*44 (37.0) |
26 (21.8) |
70 (58.8) |
|
|
26 – 35 |
14 (11.8) |
19 (16.0) |
33 (27.8) |
|
|
35 – 45 |
7 (5.9) |
7 (5.9) |
14 (11.8) |
|
|
≥ 45 |
2 (1.7) |
0 (0) |
2 (1.7) |
|
Children’s Age (months) |
6 to 12 months |
37 (31.1) |
27 (22.7) |
64 (53.8) |
|
|
13 to 24 months |
30 (25.2) |
25 (21.0) |
55 (46.2) |
|
Marital status |
Married |
11 (9.2) |
25 (21.0) |
36 (30.0) |
|
|
Single |
27 (22.7) |
5 (4.2) |
32 (26.7) |
|
|
Separated |
5 (4.2) |
6 (5.0) |
11 (9.2) |
|
|
Divorced |
2 (1.7) |
2 (1.7) |
4 (3.4) |
|
|
Windowed |
2 (1.7) |
2 (1.7) |
4 (3.4) |
|
|
**Cohabiting |
20 (16.8) |
12 (10.1) |
32 (26.9) |
|
Education Level |
Primary |
18 (15.1) |
12 (10.1) |
30 (25.2) |
|
|
High school |
17 (14.3) |
23 (19.3) |
40 (33.6) |
|
|
Vocational |
19 (16.0) |
8 (6.7) |
27 (22.7) |
|
|
University Degree |
5 (4.2) |
2 (1.7) |
7 (5.9) |
|
|
Professional School |
3 (2.5) |
2 (1.7) |
5 (2.2) |
|
|
No Formal school |
5 (4.2) |
5 (4.2) |
10 (8.4) |
|
Family Monthly Income |
<200,000 |
39 (32.8) |
32 (26.9) |
71 (59.7) |
|
|
300,000 to 400,000 |
9 (7.6) |
4 (3.4) |
13 (11.0) |
|
|
400,000 to 500,000 |
3 (2.5) |
5 (4.2) |
8 (6.7) |
|
Children in Household |
One |
25 (21.0) |
9 (7.6) |
34 (28.6) |
|
|
Two |
17 (14.3) |
17 (14.3) |
34 (28.6) |
|
|
Three |
12 (10.1) |
13 (10.9) |
25 (21.0) |
|
|
Four |
11 (9.2) |
7 (5.9) |
18 (15.1) |
|
|
Five and more |
2 (1.7) |
6 (5.0) |
8 (6.7) |
*Numbers represent counts and (percentages), respectively. **Cohabiting means living together without
legal marriage
Table 2. Cultural beliefs reported by the mothers (N = 119, except where indicated).
|
Cultural belief |
Description |
Village |
Total |
|
|
Kassanda-road |
Myanzi |
|||
|
Breastmilk is more nutritious than baby formula/other foods |
Agree |
59 (49.6) |
48 (40.3) |
107 (89.9) |
|
|
Disagree |
0 (0) |
0 (0) |
0 (0) |
|
|
Do not know |
8 (6.7) |
4 (3.4) |
12 (10.1) |
|
Giving a child water in the first weeks helps cleanse infant’s intestines |
Agree |
9 (7.6) |
7 (5.9) |
16 (13.5) |
|
|
Disagree |
14 (11.8) |
17 (14.3) |
31 (26.1) |
|
|
Do not know |
44 (37.0) |
28 (23.5) |
72 (60.5) |
|
I eat “special foods” during breast feeding |
Yes |
54 (45.4) |
38 (31.9) |
92 (77.3) |
|
|
No |
10 (8.4) |
14 (11.8) |
24 (20.2) |
|
|
Do not know |
3 (2.5) |
0 (0) |
3 (2.5) |
|
I exclusively breastfeed my baby |
Yes |
55 (46.2) |
48 (40.3) |
103 (86.5) |
|
|
No |
12 (10.1) |
4 (3.4) |
16 (13.5) |
|
Length of exclusive breastfeeding (n=117) |
2 months |
1 (0.9) |
1 (0.9) |
2 (1.8) |
|
|
3 months |
8 (6.8) |
2 (1.7) |
10 (8.5) |
|
|
4 months |
10 (8.5) |
5 (4.3) |
15 (12.8) |
|
|
5 months |
6 (5.1) |
6 (5.1) |
12 (10.2) |
|
|
6 months |
37 (31.6) |
26 (22.2) |
63 (53.8) |
|
|
Other |
5 (4.3) |
10 (8.5) |
15 (12.8) |
|
Age of introduction of water/drinks (n=117) |
1 week |
0 (0.0) |
2 (1.7) |
2 (1.7) |
|
|
2 weeks |
0 (0.0) |
1 (0.9) |
1 (0.9) |
|
|
3 weeks |
3 (2.6) |
3 (2.6) |
6 (5.2) |
|
|
1 month |
4 (3.4) |
3 (2.6) |
7 (6.0) |
|
|
3 months |
10 (8.5) |
1 (0.9) |
11 (9.4) |
|
|
4 months |
10 (8.5) |
5 (4.3) |
15 (12.8) |
|
|
5 months |
7 (6.0) |
13 (11.1) |
20 (17.1) |
|
|
6 months |
33 (28.2) |
21 (17.9) |
54 (46.1) |
|
|
Never |
0 (0.0) |
1 (0.9) |
1 (0.9) |
Numbers represent counts and (percentages)
Table 3. Reasons for breastfeeding among the mothers (n=118).
|
Reason for Breastfeeding |
Village |
Total |
|
|---|---|---|---|
|
Kassanda-road |
Myanzi |
||
|
Nutritious and healthy
Cheaper
Enjoy breastfeeding
Suggested by nurse/friends/co-workers |
23 (19.3) |
23 (19.3) |
46 (38.6) |
|
9 (13.4) |
5 (9.6) |
14 (23.0) |
|
|
5 (4.20) |
0 (0.0) |
5 (4.2) |
|
|
7 (5.9) |
1 (0.8) |
8 (6.4) |
|
|
Prevents Diseases
Closeness and bonding with baby |
10 (8.4) |
8 (6.7) |
18 (15.1) |
|
8 (6.7) |
6 (5.0) |
14 (11.7) |
|
|
Family Tradition/influence
Convenient and always ready
Encouragement from Awareness programs |
0 (0.0) |
1 (0.8) |
1 (0.8) |
|
5 (4.2) |
5 (4.2) |
10 (8.4) |
|
|
0 (0.0) |
1 (0.8) |
1 (0.8) |
|
|
Just choose to |
0 (0.0) |
1 (0.8) |
1 (0.8) |
Numbers represent counts and (percentages), respectively
Table 4. Response to other cultural beliefs among the mothers.
|
Cultural belief |
Description
|
Village |
Total |
|
|
Kassanda-road |
Myanzi |
|||
|
Weaning foods cause (n=114) |
Diarrhea |
23 (20.0) |
7 (6.1) |
30 (26.1) |
|
Wasting |
0 (0.0) |
2 (1.7) |
2 (1.7) |
|
|
Illness |
3 (2.6) |
2 (1.7) |
5 (4.3) |
|
|
|
Improved growth and wellbeing |
41 (35.7) |
36 (31.3) |
77 (67.0) |
|
I feed my child water to (n=111) |
Prevent constipation |
57 (51.4) |
35 (31.5) |
92 (82.9) |
|
|
Reduce food consumption |
9 (8.1) |
1 (0.9) |
10 (9.0) |
|
|
Do not give any water |
1 (0.9) |
7 (6.3) |
8 (7.2) |
|
|
Prevent thirst |
0 (0) |
1 (0.9) |
1 (0.9) |
Numbers represent counts and percentages respectively
Table 5. Feeding practices among toddlers aged six to 24 months.
|
Feeding practice |
Description |
Village |
Total |
||
|
Kassanda-road |
Myanzi |
||||
|
Length of breastfeeding (n=117) |
3 months |
6 (5.1) |
0 (0) |
6 (5.1) |
|
|
|
4 months |
0 (0) |
1 (0.8) |
1 (0.8) |
|
|
|
6 months |
5 (4.2) |
1 (0.8) |
6 (5.0) |
|
|
|
10 months |
3 (2.5) |
3 (2.5) |
6 (5.0) |
|
|
|
11 months |
5 (4.2) |
5 (4.2) |
10 (8.4) |
|
|
|
12 months |
13 (11) |
24 (20.3) |
37 (21.3) |
|
|
|
18 months |
8 (6.8) |
5 (4.2) |
13 (11.0) |
|
|
|
23 months |
1 (0.8) |
0 (0.0) |
1 (0.8) |
|
|
|
24 months |
25 (21.2) |
11 (9.3) |
36 (30.5) |
|
|
|
36 months |
0 (0) |
1 (0.8) |
1 (0.8) |
|
|
Age of complementary Feeding (N=119) |
2 months |
0 (0) |
1 (0.8) |
1 (0.8) |
|
|
|
4 months |
10 (8.4) |
2 (1.7) |
12 (10.1) |
|
|
|
5 months |
6 (5.0) |
1 (0.8) |
7 (5.8) |
|
|
|
6 months |
43 (36.1) |
41 (34.5) |
84 (70.6) |
|
|
|
> 6 months |
8 (6.7) |
7 (5.8) |
15 (12.5) |
|
|
Common complementary Food* (N=119) |
Starchy porridges |
|
|
|
|
|
|
Maize porridge |
9 (7.5) |
13 (10.9) |
22 (19.7) |
|
|
|
Mashed starchy vegetables |
|
|
|
|
|
|
Mashed potato |
35 (29.4) |
27 (22.7) |
62 (52.1) |
|
|
|
Mashed sweetpotato |
8 (6.7) |
2 (1.7) |
10 (8.4) |
|
|
|
Mashed pumpkin |
0 (0.0) |
1 (0.8) |
1 (0.8) |
|
|
|
Mashed plantain |
0 (0.0) |
1 (0.8) |
1 (0.8) |
|
|
|
Protein Foods |
|
|
|
|
|
|
Enkejje soup |
11 (9.2) |
4 (3.4) |
15 (12.6) |
|
|
|
Boiled egg |
4 (3.4) |
4 (3.4) |
8 (6.8) |
|
|
Common maize-blend Porridge*** (n=88) |
Maize+Grain |
|
|
|
|
|
|
Maize and millet |
31 (27.2) |
14 (12.3) |
45 (39.5) |
|
|
|
Maize+Pulses |
|
|
|
|
|
Maize and beans |
2 (1.8) |
|
4 (3.5) |
||
|
|
Maize+Protein |
|
|
|
|
|
|
Maize and Enkejje |
19 (16.7) |
11 (9.6) |
30 (26.3) |
|
|
|
Maize+Vegetable |
|
|
|
|
|
|
Maize and pumpkin |
2 (1.8) |
2 (1.8) |
4 (3.6) |
|
|
|
Maize+starchy vegetable |
|
|
|
|
|
|
Maize and cassava |
1 (0.9) |
2 (1.8) |
3 (2.7) |
|
Numbers represent counts and (percentages), respectively.
Table 6. Feeding Frequency of Maize and Maize-blended Porridges among Children aged 6 to 24 Months, Kassanda and Myanzi (N = 119, except where indicated).
|
Feeding frequency |
Description |
Village |
Total |
|
|
Kassanda-road |
Myanzi |
|||
|
Frequency of maize porridge consumption per day |
Daily |
18 (15.1) |
7 (5.9) |
25 (21.0) |
|
|
Twice a day |
27 (22.7) |
23 (19.3) |
50 (42.0) |
|
|
Three times a day |
13 (10.9) |
10 (8.4) |
23 (19.3) |
|
|
Four times a day |
3 (2.5) |
5 (4.2) |
8 (6.7) |
|
|
Five times and more a day |
0 (0.0) |
2 (1.7) |
2 (1.7) |
|
|
Never |
6 (5.0) |
5 (4.2) |
11 (9.2) |
|
Frequency of blended porridge consumption per day |
Daily |
18 (15.1) |
6 (5.0) |
24 (20.1) |
|
|
Twice a day |
23 (19.3) |
17 (14.3) |
40 (33.6) |
|
|
Three times a day |
12 (10.1) |
9 (7.6) |
21 (17.7) |
|
Feeding frequency |
Description |
Village |
Total |
|
|
Kassanda-road |
Myanzi |
|||
|
|
Four times a day |
3 (2.5) |
6 (5.0) |
9 (7.5) |
|
|
Five times and more a day |
0 (0.0) |
2 (1.7) |
2 (1.7) |
|
|
Never |
11 (9.2) |
12 (10.1) |
23 (19.3) |
|
Quantity of maize porridge consumed per day (n=114) |
0.5 cups (125 mL) |
7 (6.1) |
3 (2.6) |
10 (8.7) |
|
1.0 cup (250 mL) |
31 (27.2) |
18 (15.8) |
49 (43.0) |
|
|
1.5 cups (375 mL) |
10 (8.8) |
4 (3.5) |
14 (12.3) |
|
|
2.0 cups (500 mL) |
19 (16.7) |
17 (14.9) |
36 (31.6) |
|
|
3.0 cups (750 mL) |
0 (0.0) |
2 (1.8) |
2 (1.8) |
|
|
4.0 cups (1,000 mL) |
0 (0.0) |
3 (2.6) |
3 (2.6) |
|
|
Frequency of water given per day (n=118) |
Daily |
22 (18.6) |
21 (17.8) |
43 (36.4) |
|
Sometimes |
37 (31.4) |
27 (22.9) |
64 (54.0) |
|
|
Rarely |
8 (6.8) |
0 (0.0) |
8 (6.8) |
|
|
Never |
0 (0.0) |
3 (2.5) |
3 (2.5) |
|
Numbers represent counts and (percentages), respectively
Table 7. Source of Maize Purchased by Mothers (N=119) in Kassanda and Myanzi
|
Maize source |
Village |
Total |
|
|
Kassanda-road |
Myanzi |
||
|
Local retail shop |
25 (21.0) |
27 (22.7) |
52 (43.7) |
|
Local maize mill |
0 (0.0) |
6 (5.0) |
6 (5.0) |
|
Large Grocery store |
18 (15.1) |
5 (4.2) |
23 (19.3) |
|
Garden |
23 (19.3) |
15 (12.6) |
38 (31.9) |
Numbers represent counts and percentages respectively
Table 8. Body Mass Index of Children by Village, Kassanda-road, Myanzi.
|
Village |
Kassanda-road |
Myanzi |
Total |
|
Number of children assessed: |
60 |
59 |
119 |
|
Underweight (< 5th percentile) |
2% |
3% |
3% |
|
Normal BMI (5th - 85th percentile) |
88% |
81% |
85% |
|
Overweight or obese (≥ 85th percentile) |
10% |
15% |
13% |
|
Obese (≥ 95th percentile) |
2% |
8% |
5% |
Figure Legends:
Figure 1. Location of Study Area - Kassanda-road and Myanzi Villages.
Figure 2. The Administrative Layout of the Study Area.
Figure 3. Reasons for Early Complementary Feeding before Six Months.
Figure 4. Factors Influencing the Choice of Complementary Food among Children 6-24 Months in Kassanda-road and Myanzi.
Figure 5. Importance of Nutrition when Selecting a Complementary Food among Children 6-24 Months in Kassanda-road and Myanzi.
Figure 6. Body Mass Index of Children by Gender, Kassand-road and Myanzi.

The Roles of Choline in Maintaining Optimal Health
The Effects of Intake of Bread with Treated Corn Bran Inclusion on Postprandial Glyceamic Response
Food Waste throughout the Food Production Continuum – Water Food and Energy Nexus
Use of Lightly Potassium-Enriched Soy Sauce at Home Reduced Urinary Sodium-to-Potassium Ratio
A Different Type of Critical Migration
PRECEDE: A Conceptual Model to Assess Immigrant Health
Walking Together: Supporting Indigenous Student Success in University
Cosmetic Surgery and Body Image in Race/Ethnic Minorities
Our articles most useful
Adrian Taylor and Marica Bakovic*
Published : June 21, 2019
Journal of Food & Nutritional Sciences
Zhimin Cui, Lynne Kennedy, Weili Li*
Published : September 30, 2019
Journal of Food & Nutritional Sciences
Elena Castell-Perez*, Rosana G. Moreira, Hal S. Knowles, III
Published : October 01, 2019
Journal of Food & Nutritional Sciences
Nagako Okuda, Makoto Miura, Kazuyoshi Itai, Takuya Morikawa, Junko Sasaki, Tamami Asanuma, Mikako Fujii, Akira Okayama
Published : March 27, 2019
Journal of Food & Nutritional Sciences